Talk to Lawyer
Mark Kopec Now
Mark Kopec Now


Cardiac tamponade is a life-threatening medical condition that occurs when fluid builds up in the space between the heart muscle and the outer covering of the heart. This accumulation of fluid creates extreme pressure, preventing the heart’s ventricles from expanding fully. When the heart cannot expand, it cannot fill with enough blood, leading to a drastic drop in blood pressure and, eventually, systemic organ failure. Baltimore cardiac tamponade lawyer Mark Kopec provides you with this article to explain the various aspects of this condition and potential medical malpractice claims.
In the context of medical care, cardiac tamponade is often a “can’t miss” diagnosis. Because it can progress rapidly from mild discomfort to cardiac arrest, healthcare providers must act with extreme urgency. When they fail to do so—or when their actions cause the condition—it often leads to medical malpractice litigation.
To understand tamponade, one must understand the pericardium. The heart is in a double-walled sac, which is the pericardial sac.
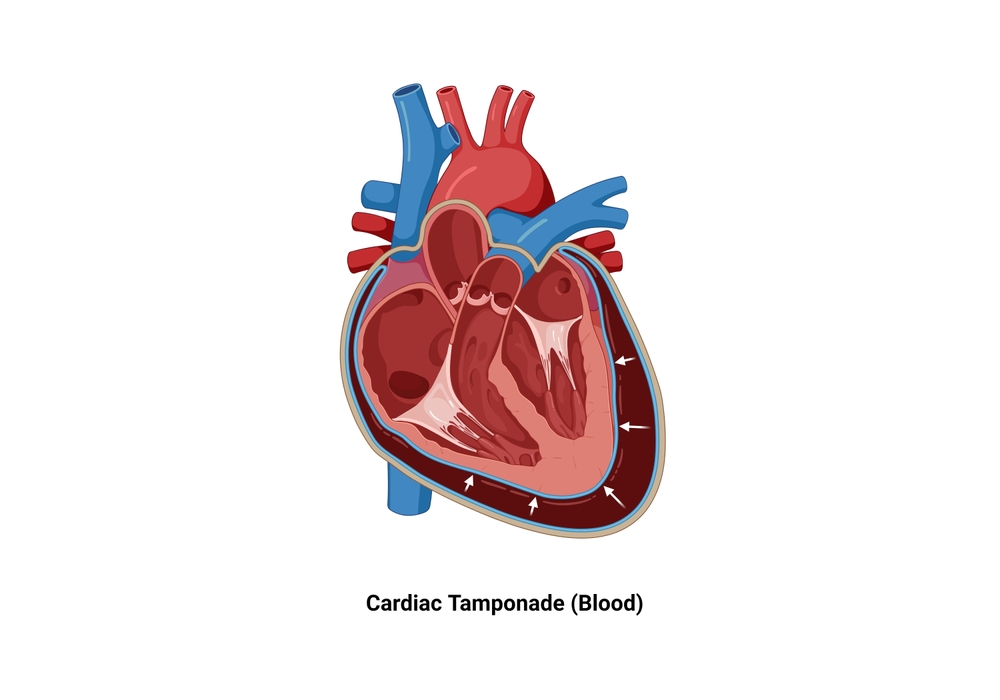
In cardiac tamponade, this cavity fills with excess fluid (blood, pus, or effusion). Because the outer parietal pericardium is relatively stiff and inelastic, it cannot stretch quickly. As fluid volume increases, the pressure is directed inward, then compressing the heart chambers.
Cardiac tamponade can result from a variety of underlying issues, generally ranging from chronic illness to acute trauma.
Common Causes:
Risk Factors:
Patients with end-stage renal disease (uremia), those on blood thinners (anticoagulants), and individuals with autoimmune diseases like Lupus are at a higher risk for developing pericardial effusions that can lead to tamponade.
The clinical presentation of cardiac tamponade can be subtle at first but usually escalates quickly. Physicians are trained to look for a classic set of three signs known as Beck’s Triad:
Other symptoms include shortness of breath (dyspnea), rapid heart rate (tachycardia), lightheadedness, and pulsus paradoxus—a significant drop in blood pressure during inhalation.
If a patient presents with symptoms in an Emergency Room, the primary physician involved will be an Emergency Medicine Physician. However, a Cardiologist is usually consulted immediately for definitive diagnosis and management.
Diagnostic Tests:
Baltimore cardiac tamponade lawyer Mark Kopec will evaluate your diagnosis and advise you on a potential medical malpractice claim.
Treatment is focused on removing the fluid to relieve pressure. This is a surgical emergency.
Physicians Involved:
Treatment Methods:
If treated immediately, many patients recover fully. However, if there is a delay, the outcomes can be catastrophic:
Medical malpractice claims involving cardiac tamponade generally fall into two categories: errors in causation and errors in response.
These claims arise when a healthcare provider’s negligence directly results in the tamponade.
These claims focus on the “failure to diagnose” or “failure to treat” in a timely manner.
In these cases, the legal “standard of care” is the focal point. An expert witness (usually a board-certified cardiologist) must testify that a competent doctor in the same circumstances would have recognized the signs and acted faster.
If you have any concerns or questions about cardiac tamponade, then visit our free consultation page or video. Then contact the Kopec Law Firm at 800-604-0704 to speak directly with Attorney Mark Kopec. He is a top-rated Baltimore medical malpractice lawyer. The Kopec Law Firm is in Baltimore and pursues cases throughout Maryland and Washington, D.C.